
ACL, or anterior cruciate ligament, injuries are one of the most common—and perhaps most devastating—sports injuries. Aside from the significant physical trauma, they often lead to a lengthy interruption in sports participation and require an intensive course of rehabilitation.
While we know that participation in sport comes with inherent risks, when a particular injury becomes highly prevalent, as is the case with ACL injuries, prevention becomes a compelling piece of the puzzle.
Prevention begins with identifying and addressing modifiable factors that may influence injury risk. Historically, much of the discussion surrounding ACL prevention has focused on movement mechanics, neuromuscular control and strength. More recently, researchers and clinicians have also explored the influence of mobility and movement capacity throughout the lower-extremity kinetic chain.
Because the knee is an intermediate joint, the forces acting on it are influenced by both the hip and the ankle. One area that has received considerable attention is the relationship between hip mobility—particularly hip internal rotation—and movement strategies commonly associated with ACL injury mechanisms (1).
While factors such as muscle activation patterns, neuromuscular control and movement technique undoubtedly influence how athletes move, fundamental physical qualities such as joint mobility also contribute to how efficiently forces are absorbed and redistributed throughout the body.
Movements such as cutting, landing and deceleration have long been identified as common mechanisms associated with ACL injury. Rather than asking whether hip mobility directly contributes to ACL injury, a more useful question may be:
How does hip mobility influence an athlete’s ability to manage these demands?
Let’s explore the role of the hip from that kinetic-chain perspective.
Enjoyed this video? Make sure you subscribe to our YouTube channel!
ACL INJURIES – WHAT YOU NEED TO KNOW
To understand why hip mobility may matter, we first need to understand how forces are managed throughout the lower-extremity kinetic chain during these injury mechanisms.
While traumatic ACL injuries may result from contact with an opponent, non-contact mechanisms are about 80% more likely to cause an ACL injury (2). These non-contact injuries have been described as a combination of multiple plane forces acting collectively on the knee and involve the foot and ankle complex, the knee and the hip.
Perhaps the most recognized mechanism of injury is valgus loading such as when the individual takes off from the planted foot and internally rotates with the aim of suddenly changing direction:

Here is a video that shows this mechanism quite well: ACL Injury
Similar mechanisms have also been identified in landing tasks.
Globally, non-contact ACL injuries seem to be impacted by HOW forces are absorbed, distributed and transferred along the lower limb kinetic chain
Biomechanical inefficiency of this force distribution may contribute to increased ACL loading and eventually, failure.
The kinetic chain is composed of a series of interrelated sequentially activated segments, where movement of one segment affects the proximal and distal segments. Distally, the foot and ankle complex play an important role in absorbing and dissipating ground reaction forces as the foot impacts the ground. Appropriate ankle mobility is also important in affording us the capacity to absorb torsional forces such as those created when changing directions or decelerating.
As such, restoring or improving foot and ankle function is a crucial part of any rehab or prevention strategy. Make sure you read this article to learn how to restore specific ankle mobility for prevention.
Recently, more attention has been shifted proximally to the hip and the influence of its position on ACL injuries.
HIP INTERNAL ROTATION AS A MOVEMENT RESOURCE
The lower limb acts much like a shock absorber during athletic movement. As an athlete takes a step, shifts weight onto one leg, decelerates, lands from a jump or changes direction, forces must be absorbed and redistributed throughout the entire kinetic chain.
During these athletic tasks, the pelvis naturally rotates over the stance femur while the trunk continues moving over the base of support. This “pelvis-over-femur” relationship is a normal component of force absorption and allows the lower extremity to dissipate rotational forces rather than concentrating them at a single joint.
This is where hip internal rotation becomes particularly interesting.
Rather than viewing hip internal rotation as a direct cause-and-effect relationship with ACL injury, it may be more useful to view it as a movement resource.
During cutting, landing and deceleration tasks, the pelvis naturally moves and rotates over the stance femur while the trunk continues moving over the base of support. This rotational movement helps absorb and redistribute force throughout the lower extremity.
Hip internal rotation contributes to this process.
When adequate hip internal rotation is available, the athlete may have more options for distributing force efficiently throughout the kinetic chain. When hip internal rotation is limited, the athlete may still complete the task successfully, but may do so using different movement strategies.
These strategies may include greater hip adduction, altered trunk mechanics, changes in tibial rotation or greater dynamic knee valgus.
Importantly, this does not mean that hip stiffness automatically causes ACL injury. Rather, it suggests that hip mobility may influence how forces are managed during athletic movement.
The question is whether the athlete possesses the movement resources necessary to efficiently absorb and redistribute force during the demands of sport.

WHAT DOES LIMITED HIP MOBILITY LOOK LIKE?
As mentioned earlier in this article, the concept of the kinetic chain relies on a series of interrelated body segments working together to absorb, distribute and manage force. Movement occurring at one segment will inevitably influence what occurs above and below it.
This is particularly true of the knee, which acts as an intermediate joint between the foot and ankle complex below and the hip and pelvis above. As a result, the loads experienced by the knee are often influenced by the movement options available throughout the rest of the lower-extremity kinetic chain.
When one segment contributes less to a movement task because of mobility, strength or motor-control limitations, other segments may be required to contribute more. This does not necessarily mean injury will occur, but it may influence how forces are distributed and how movement strategies are organized.
Many of you may be familiar with movement screening, which uses global movement patterns to observe how athletes interact with their environment.
While we should avoid making direct assumptions about injury risk based on any single movement screen, these assessments can provide valuable information about where movement resources may be limited, restricted or asymmetrical.
The Multisegmental Rotation Screen is one example. It allows us to observe the contribution of the feet, ankles, hips, pelvis and trunk to a rotational movement pattern. Given the important role rotation plays in force absorption during cutting, landing and deceleration, it provides a useful starting point when evaluating an athlete’s overall movement capacity.

When rotating to the left, as depicted in the picture above, the left foot will supinate and the right foot will pronate. The left hip will be in a position of internal rotation while the right hip will be in external rotation. The pelvis should rotate 50 degrees. When you assess this on both sides, you are looking at symmetry and effort. For example, you might find limited rotation to the left side when compared to the right side. If you did the test sitting and found that rotation was no longer restricted, you know something is going on in the ankles or hips and would explore that further in your assessment.

With regards to hip rotation, a great way to assess the hip specifically for hip internal rotation range of motion is to place the individual in a prone position and allow the hip to fall into internal rotation as depicted in the image below:
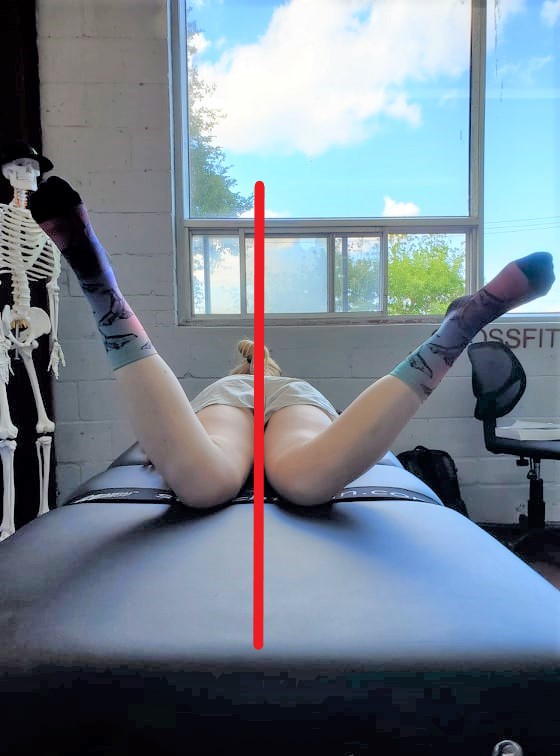
A « normal » range for hip internal rotation is about 30-40 degrees, but really you are most concerned with side-to-side differences.
While you could assess rotation in a supine position with the hip and knee flexed to 90 degrees, this prone position allows you to observe whether the weight of the lower leg can bring the hip into internal rotation.
A hip that demonstrates very limited internal rotation may have fewer movement options available during rotational athletic tasks.
By the way, this is also a great way to assess for a very mobile hip (or low stiffness), but that will be the subject of another article.
Of course, identifying limited hip internal rotation is only the beginning. Assessment should never be viewed as an endpoint. Once we identify a limitation, our objective becomes restoring that movement resource and progressively teaching the athlete how to use it under increasing loads and athletic demands.
MAKE SURE YOU WATCH THE MAIN VIDEO OF THIS ARTICLE FOR MORE ON THESE ASSESSMENTS AND OTHERS!
RESTORING MOVEMENT CAPACITY
Numerous risk factors for ACL injury have been presented in the literature. In fact, the International Olympic Committee has identified external, internal, hormonal and biomechanical factors that may contribute to ACL injury risk.
While many of these factors are difficult or impossible to modify, movement capacity is something we can influence through rehabilitation and training.
If hip internal rotation is limited, restoring mobility may provide the athlete with additional movement options. However, mobility alone is rarely the end goal. Once mobility has been restored, athletes must develop the ability to use that mobility under progressively greater demands. This includes developing pelvis-over-femur control, rotational strength, force absorption capacity and eventually the ability to manage movement under speed, fatigue and unpredictability.
In other words, restoring range of motion simply gives the athlete access to a position. Rehabilitation and training are what develop the capacity to control that position.
Whether our goal is injury prevention, rehabilitation or performance enhancement, our role as therapists and trainers is not simply to improve mobility. Our role is to provide athletes with the resources they need to efficiently absorb, distribute and manage force during the complex demands of sport.
Ultimately, mobility does not prevent injury. It simply provides another movement option.
Rehabilitation and training are what develop the capacity to use that option when it matters most.
REFERENCES
- Bittencourt, N., Ocarino, J., Mendonça, L., Hewett, T., & Fonseca, S. (2012). Foot and Hip Contributions to High Frontal Plane Knee Projection Angle in Athletes: A Classification and Regression Tree Approach. Journal Of Orthopaedic & Sports Physical Therapy, 42(12), 996-1004. doi: 10.2519/jospt.2012.4041
- Krosshaug, T., Nakamae, A., Boden, B. P., Engebretsen, L., Smith, G., Slauterbeck, J. R., Hewett, T. E., & Bahr, R. (2007). Mechanisms of anterior cruciate ligament injury in basketball: video analysis of 39 cases. The American journal of sports medicine, 35(3), 359–367.
- Kianifar, R., Lee, A., Raina, S., & Kulic, D. (2017). Automated Assessment of Dynamic Knee Valgus and Risk of Knee Injury During the Single Leg Squat. IEEE journal of translational engineering in health and medicine, 5, 2100213. https://doi.org/10.1109/JTEHM.2017.2736559

Mai-Linh Dovan M.SC., CAT(C)
Certified Athletic Therapist
Founder of Rehab-U


… [Trackback]
[…] Read More here on that Topic: rehab-u.com/hip-stiffness-is-a-risk-factor-for-acl-injury/ […]
… [Trackback]
[…] Here you will find 85914 additional Information on that Topic: rehab-u.com/hip-stiffness-is-a-risk-factor-for-acl-injury/ […]
… [Trackback]
[…] Here you can find 10699 additional Information on that Topic: rehab-u.com/hip-stiffness-is-a-risk-factor-for-acl-injury/ […]
… [Trackback]
[…] Find More here to that Topic: rehab-u.com/hip-stiffness-is-a-risk-factor-for-acl-injury/ […]
… [Trackback]
[…] Read More here on that Topic: rehab-u.com/hip-stiffness-is-a-risk-factor-for-acl-injury/ […]
… [Trackback]
[…] There you can find 113 more Info to that Topic: rehab-u.com/hip-stiffness-is-a-risk-factor-for-acl-injury/ […]
… [Trackback]
[…] Find More to that Topic: rehab-u.com/hip-stiffness-is-a-risk-factor-for-acl-injury/ […]
… [Trackback]
[…] There you can find 58409 additional Information on that Topic: rehab-u.com/hip-stiffness-is-a-risk-factor-for-acl-injury/ […]
… [Trackback]
[…] There you can find 20857 more Information on that Topic: rehab-u.com/hip-stiffness-is-a-risk-factor-for-acl-injury/ […]
… [Trackback]
[…] Read More Info here to that Topic: rehab-u.com/hip-stiffness-is-a-risk-factor-for-acl-injury/ […]
… [Trackback]
[…] Here you can find 35679 additional Info to that Topic: rehab-u.com/hip-stiffness-is-a-risk-factor-for-acl-injury/ […]
… [Trackback]
[…] Read More to that Topic: rehab-u.com/hip-stiffness-is-a-risk-factor-for-acl-injury/ […]
… [Trackback]
[…] There you will find 38196 more Info to that Topic: rehab-u.com/hip-stiffness-is-a-risk-factor-for-acl-injury/ […]
… [Trackback]
[…] Find More Info here on that Topic: rehab-u.com/hip-stiffness-is-a-risk-factor-for-acl-injury/ […]
… [Trackback]
[…] Find More here to that Topic: rehab-u.com/hip-stiffness-is-a-risk-factor-for-acl-injury/ […]
… [Trackback]
[…] Find More to that Topic: rehab-u.com/hip-stiffness-is-a-risk-factor-for-acl-injury/ […]
… [Trackback]
[…] Find More on that Topic: rehab-u.com/hip-stiffness-is-a-risk-factor-for-acl-injury/ […]
… [Trackback]
[…] Read More to that Topic: rehab-u.com/hip-stiffness-is-a-risk-factor-for-acl-injury/ […]
… [Trackback]
[…] Find More to that Topic: rehab-u.com/hip-stiffness-is-a-risk-factor-for-acl-injury/ […]
… [Trackback]
[…] Find More here on that Topic: rehab-u.com/hip-stiffness-is-a-risk-factor-for-acl-injury/ […]
… [Trackback]
[…] Here you will find 84088 more Information to that Topic: rehab-u.com/hip-stiffness-is-a-risk-factor-for-acl-injury/ […]
… [Trackback]
[…] Find More on on that Topic: rehab-u.com/hip-stiffness-is-a-risk-factor-for-acl-injury/ […]
… [Trackback]
[…] Find More Info here to that Topic: rehab-u.com/hip-stiffness-is-a-risk-factor-for-acl-injury/ […]
… [Trackback]
[…] Find More Info here to that Topic: rehab-u.com/hip-stiffness-is-a-risk-factor-for-acl-injury/ […]
… [Trackback]
[…] Find More Information here on that Topic: rehab-u.com/hip-stiffness-is-a-risk-factor-for-acl-injury/ […]
… [Trackback]
[…] There you will find 77094 additional Information on that Topic: rehab-u.com/hip-stiffness-is-a-risk-factor-for-acl-injury/ […]
… [Trackback]
[…] Read More Information here on that Topic: rehab-u.com/hip-stiffness-is-a-risk-factor-for-acl-injury/ […]
… [Trackback]
[…] Info to that Topic: rehab-u.com/hip-stiffness-is-a-risk-factor-for-acl-injury/ […]
… [Trackback]
[…] Info to that Topic: rehab-u.com/hip-stiffness-is-a-risk-factor-for-acl-injury/ […]
… [Trackback]
[…] There you can find 39572 additional Info on that Topic: rehab-u.com/hip-stiffness-is-a-risk-factor-for-acl-injury/ […]
… [Trackback]
[…] Find More to that Topic: rehab-u.com/hip-stiffness-is-a-risk-factor-for-acl-injury/ […]
… [Trackback]
[…] Here you can find 97415 additional Information to that Topic: rehab-u.com/hip-stiffness-is-a-risk-factor-for-acl-injury/ […]
… [Trackback]
[…] Information on that Topic: rehab-u.com/hip-stiffness-is-a-risk-factor-for-acl-injury/ […]